Treacher Collins Syndrome
What is Treacher Collins Syndrome?
AB Collins Syndrome also called Treacher Collins syndrome (TSC) refers to an autosomal dominant congenital disorder whose characteristics are the craniofacial deformities mostly of the ears, eyes, jawbone and cheekbone. People affected by this syndrome have normal intelligence.
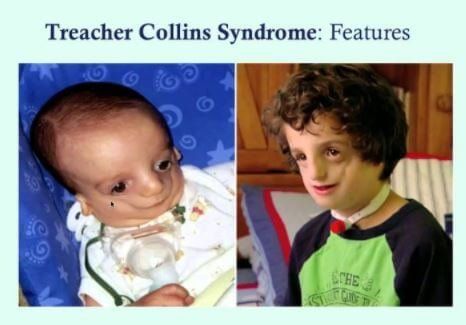
The typical characteristics are a small lower jaw (micrognathia), downward slanting eyes, the drooping section of the lateral lower eyelids, malformed or absent ears and underdeveloped zygomatic bones among others. However, these characteristics vary from one affected person to another and they can lead to breathing, seeing or hearing related problems.
It is named after an English surgeon and ophthalmologist called Edward Treacher Collins who first explained its essential traits in 1900.
Causes
The Treacher Collins Syndrome is often caused by a mutation in TCOF1 gene, which accounts for 81 to 93% of the cases, but can also be as a result of POLRIC or POLRID mutations, which account for 2% of all cases. All these mutations involve genes in the development of the ribosomes assembly as well as pharyngeal arches, which make the syndrome a ribosomopathy.
The genetic cause of the syndrome is unknown in individuals who have an unidentified mutation. Though imaging can be employed to determine specific symptoms, TCS is normally diagnosed through physical examination.
Since the syndrome is incurable, its symptoms are manageable with the use of hearing aids, reconstructive surgery, and other assistive practices and devices. The syndrome occurs in approximately one in 50,000 births in Europe. 4
Signs & Symptoms
The signs and symptoms of Treacher Collins syndrome vary from one person to another with some people remaining undiagnosed since they are mildly affected while others suffer severe facial involvement as well as life-threatening compromises. Most of the signs are asymmetrical and can be recognized at birth.
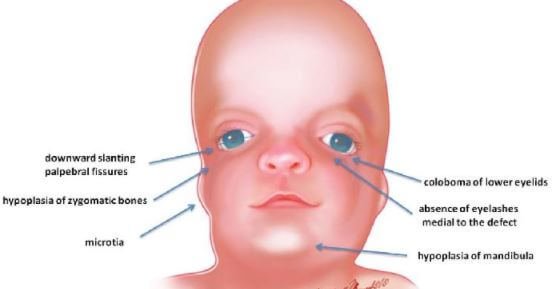
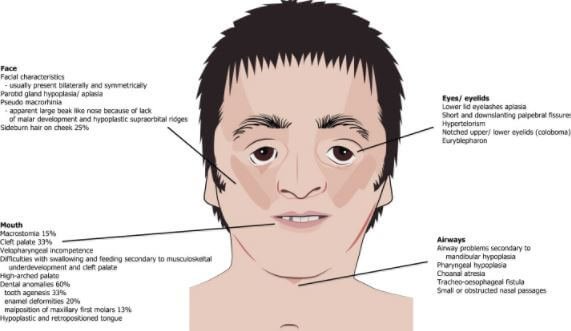
- Hypoplasia: This is the most common symptom of the syndrome. It involves the underdevelopment of lower jaw (mandible) also known as micrognathia and zygomatic bone referred to as “malar hypoplasia”. All these could be accompanied by glossoptosis.
- Mandibular hypoplasia can lead to disorientation in the alignment of jaws and the teeth, a condition called malocclusion and can lead to severity in swallowing and breathing problems. Cheeks get a sunken appearance due to the underdevelopment of the zygomatic bone.
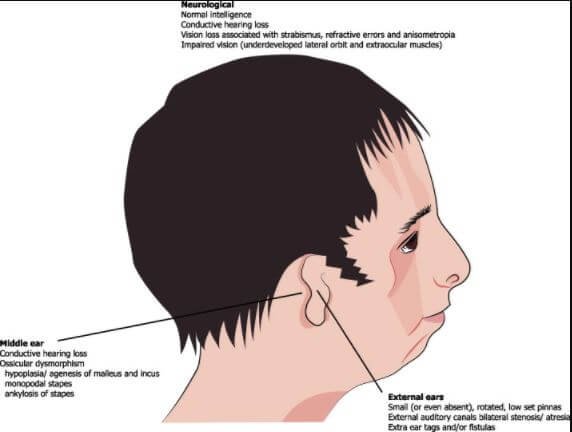
- The diminishing, rotation, malformation or absence of the external ear, pinna, is another symptom of one suffering from TSC. It is also characterized by the symmetric or bilateral narrowing (stenosis) or absence (atresia) of the external auditory canals
- where most often, there is misshapen of the middle ear cavity and ossicles. These malformations and abnormalities cause a conductive hearing loss in most people with TSC. The malformations of the inner ears are rarely referred to.
- Eye problems are also a sign and symptom of TSC. These eye complications include notches in the lower eyelid (colobomata), a partial or total absence of eyelashes on the lower lid, drooping of the upper and lower eyelids (ptosis), narrowing of tear ducts (dacrostenosis) and the downward angle of eyelids.
- One can also suffer a loss of vision associated with strabismus, anisometropia, and refractive errors or even severe dry eyes, an implication of frequent eye infections and lower eyelid abnormalities.
- Bitemporal narrowing of brachycephaly is observed with cleft palate being common despite the fact that an abnormally shaped skull is not distinctive.
- Dental anomalies: these are observable in 60% of TCS affected people which includes tooth agenesis, discoloration (enamel opacities), wide teeth spacing and misplacement of maxillary first molars. Malocclusion can occur due to the combination of mandible hypoplasia and dental anomalies which can cause complications in the ability to close the mouth as well as food intake problems.
- Less severe signs and symptoms can also cause breathing problems as well as sleep apnea. Narrowing or absence of choanae (choanal atresia/stenosis) which is the internal opening of nasal passages may occur. Airway can also narrow due to underdevelopment of pharynx (pharyngeal hypoplasia).
- There is also the less seen signs and symptoms of TCS such as high-arched palate, nasal deformities, cleft palate, hypertelorism, preauricular displacement of hair, congenital heart defects and notched upper eyelid.
However, it is important to note that people affected with TCS have normal intelligence. Quality life of TCS affected people may be affected by psychological and social problems attributed to facial deformities.
Diagnosis
The diagnosis of Treacher Collins Syndrome relies upon clinical and radiographic findings as the prenatal diagnosis is not reliable. The condition is first observable during a clinical examination. However, clinical examination findings can resemble other diseases hence making the diagnosis difficult.
For comprehensive and stage-based differentiation of diseases, there was the development of OMENS classifications. OMENS is a description of five distinct dysmorphic manifestations called orbital asymmetry, mandibular hypoplasia, auricular deformity, nerve development and soft-tissue disease.
For prenatal diagnosis, chorionic villus sampling (amniocentesis) is used to detect mutations in the main genes that are responsible for TSC except for rare mutations. Craniofacial deformities in pregnancy can be detected using ultrasonography though milder cases may not be detected.
Treatment
The treatment of TCS condition involves the intervention of multidisciplinary professionals. Breathing and feeding are the main concerns as a result of hypoplasia of mandibular as well as obstruction of hypopharynx by the tongue.
Tracheostomy may be required for maintenance of adequate airway as well as agastrostomy, which ensures adequate caloric intakes while taking care of the airway. Corrective surgical operations can be performed to the face at various ages according to the developmental state. The treatment guidelines are as follows:
- Repair takes 9-12 months if cleft palate is present (Read Gastroschisis repair). A polysomnography with a palatal place is required before surgery. Postoperative situations may be predicted giving an insight on chances of development of sleep apnea (OSAS) after the operation.
- Bone conduction amplification, speech therapy and educational intervention to prevent language/speech problems are done to treat hearing loss. Bone-anchored hearing aid can also be used.
- Complete development of cranio-orbitozygomatic bone allows the performance of zygomatic and orbital reconstruction (5-7 years). Autologous bone graft is often used in children. Lipofilling, in combination with this transplantation, can be used in periorbital are for optimal results of reconstruction. Lower eyelid coloboma reconstruction includes the use of elevated myocutaneous flap closing the eyelid defect.
- At eight years of age, external ear reconstruction can be done and at times, middle ear or external auditory canal can be treated as well.
- Nose reconstruction can be performed where necessary after 18 years of age and after orthognatic surgery is done.
- Teeth should be under the supervision of orthodontist, when cutting, to ensure no abnormalities happen. Appropriate action is taken in case abnormalities such as dislocation or teeth overgrowth are detected.
- Orthognatic treatments take place after 16 years of age since by then all teeth are in place and the jaw and denture are fully mature. The level of obstruction is determined by endoscopy of upper airways once OSAS is detected. Mandibular advancement can act as an effective method of improving both breathing and aesthetics while a chinplasty restores the profile only.
- Maxillomandibular reconstruction can be performed at different ages as classified below:
- 13-16 years: Type I (mild) and Type IIa (moderate)
- Type IIb (moderate to severe malformation) done at skeletal maturity.
- Due to facial skeletal maturity, the facial soft tissues’ contour requires correction at a later stage. Correction of facial soft tissue contours is improved by use of microsurgical methods such as free flap transfer. Lip filling is another method used to improve the contour of facial soft tissues, for instance, it is used in the reconstruction of eyelids.
Pictures
Reference List
- The Treacher Collins syndrome (TCOF1) gene product is involved in ribosomal DNA gene transcription by interacting with upstream binding factor. Retrieved from https://www.research.manchester.ac.uk/portal/en/publications/
- Treacher Collins Syndrome. Retrieved from https://ghr.nlm.nih.gov/condition/treacher-collins-syndrome
- Treacher Collins Syndrome. Retrieved from https://en.wikipedia.org/wiki/Treacher_Collins_syndrome
- Mutations in the Treacher Collins Syndrome Gene Lead to Mislocalization of the Nucleolar Protein Treacle. Retreived from https://academic.oup.com/hmg/article/7/11/1795/2357124/Mutations-in-the-Treacher-Collins-Syndrome-Gene
- Treacher Collins syndrome. Retrieved from https://www.betterhealth.vic.gov.au/health/conditionsandtreatments/treacher-collins-syndrome
- www.faces-cranio.org/Disord/Treacher.htm
- https://www.medicalnewstoday.com/articles/320306.php
- kidshealth.org/en/parents/tcs.html
- https://ccakids.org/treacher-collins-syndrome.html
- www.chop.edu/conditions-diseases/treacher-collins-syndrome