Gastroschisis
Definition
Gastroschisis refers to a rare birth problem that is characterized by a specific defect affecting the anterior portion of the abdominal wall, in which the abdominal intestinal contents are noted to be freely protruding outside a baby’s body.

These contents are not covered by any overlaying sac and not protected by any peritoneum; placing it at risk for irritation, swelling and possible damage with undue exposure. Its size is mostly smaller than 5cm.
The defect of the abdominal wall in babies with gastroschisis is found at the junction where the umbilicus and the normal skin meets together; where a hole is developed mostly on the right side, allowing the intestines of the baby to be coming out of the abdomen. This disorder arises when the woman is on its fourth week of the pregnancy period. The incidence of this problem is approximately 1 case for every 2000 births.
Symptoms of Gastroschisis
Clinical manifestations of gastroschisis include:
- Presence of lump in the abdomen area
- Intestinal contents are sticking out of the body through an abdominal hole commonly observed on the right side of the umbilical cord area
- Protruded bowel contents appears unprotected posing a risk for irritation, possible swelling and some undue damage
Causes
The exact cause of gastroschisis is not yet known; however, there a number of hypothetical studies which tries to support its pathology. This herniation disorder involving the gastrointestinal contents is not related with any congenital anomaly.
A woman who delivers a newborn baby with gastroschisis does not mean that the succeeding deliveries will always be another baby with the same problem. An elevated level of the maternal serum alpha-fetoprotein is linked with the occurrence of gastroschisis.
At the time of the fourth week of the pregnancy, it has been noted that the lateral body folds are moving ventrally, which will then fuse in the midline in order to form the anterior body wall area.
An incomplete fusion can result in impairment that allows abdominal contents to protrude freely along the small opening in the abdominal wall. This herniation of the bowel passes through the rectus muscle, which is lying on the right side of the umbilicus.
Gastroschisis can be complicated by the following conditions:
- Polyhydramnios
- Gastroesophageal reflux disease
- Hirschsprung’s disease
- Malabsorption and intestinal dysmotility
Predisposing risk factors which might lead to gastroschisis:
- Taking aspirin medication during pregnancy
- Change in paternity which pertains to childbearing involving different fathers
Diagnosis
The physical examination of the baby by an attending physician or pediatrician is already enough to diagnose a problem of gastroschisis.
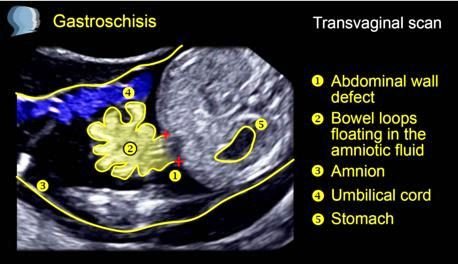 Image 2 – Gastroschisis ultrasound doppler scan
Image 2 – Gastroschisis ultrasound doppler scan
Prenatal procedures which are often done to confirm the diagnosis of gastroschisis:
- Antenatal sonography can detect gastroschisis in the second trimester of the pregnancy. It also allows some fetal interventions as necessary, in uteru transfer whenever possible, planned delivery in a unit that renders special services, and performing parental antenatal counseling to discuss the prognosis and possible outcomes of the problem towards the baby.
- Routine blood tests to assess and evaluate the maternal alpha-fetoprotein level that becomes increased in cases of gastroschisis.
Sonographic results that suggests an existing gastroschisis problem:
- Exteriorized bowel contents in relation to the anterior abdominal wall
- Presence of multiple loops of bowel contents
- Thickened bowel noted to be freely floating in the amniotic fluid
Treatment
The main goal is to perform a surgical procedure in order to put back inside the abdomen all protruding intestinal contents from an abnormal abdominal wall opening.
Primary repair is a single surgical procedure needed to bring back bowel contents inside the abdomen and closing the opening or hole of the abdominal wall involved.
Staged repair requiring multiple surgeries needed in instances when the baby has a very large amount of bowel contents that are protruding outside the body, taking about three to ten days or even longer.
Application of protective “silo” on the abdominal contents which are outside the abdomen, followed by slow gentle pressure to make the herniated intestines placed back inside the abdominal cavity.
Postoperative care for the baby:
- IV therapy
- Medications for pain and comfort
- Antibiotics to prevent infection
- Breast milk or special formula feeding once the bowel starts to function
Gastroschisis Vs Omphalocele
Omphalocele is a defect of the anterior abdominal wall specifically at the base of the umbilical cord, in which the herniated organs are protected and covered by a parietal peritoneum; whereas in gastroschisis, the herniated abdominal contents are freely protruding and without any protective cover.
Omphalocele:
- Careful examination is done to detect associated problems like chromosomal abnormalities, congenital heart disease or any other linked malformations
- Babies with intact omphalocele does not lead to respiratory distress, except in the presence of pulmonary hypoplasia
- IV solutions are started
- Nonadherent dressing is used to cover an omphalocele sac
- Preoperative antibiotics might be given
- Closure of a small to moderate-sized omphalocele
- Ruptured omphalocele is treated similarly like gastroschisis
- Giant omphalocele is treated with topical agents for a period of several weeks
Gastroschisis:
- Gastric decompression can help with respiratory distress, or some may need an endotracheal intubation
- Intravenous fluid bolus are given to correct fluid and electrolyte imbalance and some heat loss
- Baby is placed under a radiant heater
- Eviscerated intestine is placed on top of the baby’s abdomen
- Kerlix can be used to wrap the eviscerated intestinal contents to prevent traction application upon the mesenteric bowel
- Urinary catheter insertion is done to monitor urine output
- Rectal examination done to dilate the anal canal
- Broad spectrum antibiotics are given to prevent the peritoneal cavity to be contaminated
- Central venous line to provide adequate parenteral nutrition
Prognosis
The recovery of the affected baby is usually good once the abdominal cavity is considered large enough to take in the herniated abdominal contents. An additional surgery might be necessary in the presence of a very small abdominal cavity which might lead to some complications. Survival rate has increased to 90% of the cases with the availability of some current advancement in terms of surgical techniques done to resolve the problem.
Pictures



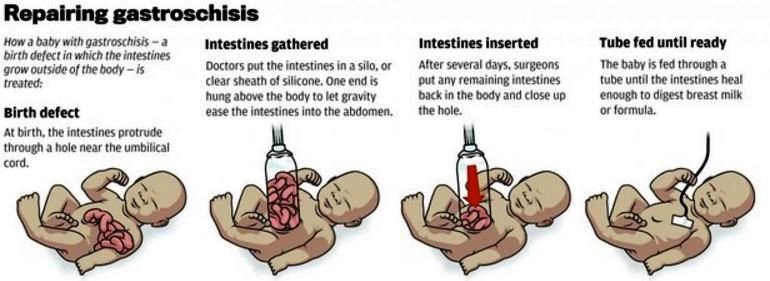
Image 6 – Repair of Gastroschisis (steps)
References:
- http://emedicine.medscape.com/article/975583-overview
- After Surgery for Gastroschisis at http://www.seattlechildrens.org/medical-conditions/digestive-gastrointestinal-conditions/gastroschisis-treatment/
- https://www.nlm.nih.gov/medlineplus/ency/article/000992.htm
- Le Tao, Bhushan Vikas, Sochat Mathew (2015). First AID for the USME1 Step 1 2015. New York: McGraw Hill Education.
- Mac Bird T, Robbins JM, Druschel C, Cleves MA, Yang S, Hobbs CA, et al. (2009). “Demographic and environmental risk factors for gastroschisis and omphalocele in the National Birth Defects Prevention Study”. J Pediatr Surg 44 (8): 1546–51.
- Schnur J, Dolgin S, Vohra N, Soffer S, Glick R (2008). Pitfalls in prenatal diagnosis of unusual congenital abdominal wall defects. J Matern Fetal Neonatal Med. 21(2):135-139.