Inverted Uterus
What is an Inverted Uterus?
An inverted uterus is a fatal complication that usually happens when excessive manipulation is done with the uterus after the delivery of a newborn baby, and this is also known as uterine inversion. This occurs in the failure of the placenta to separate itself from the uterus in the delivery process, pulling in its inner portion and reversing the organ and turned inside out, with an 85% maternal chance of survival rate.
Uterine inversion is considered a rare obstetrical problem associated with pregnant women and mostly noted during labor and delivery particularly in the second stage, where members of the health team has to be vigilant with its assessment findings, have a timely diagnosis of the problem and implement standard measures to prevent the risk of postpartum bleeding as a consequence.
The association of this uterine problem is very rarely observable among non-pregnant women, although it may occur together with some existing tumors or in some cases of prolapsing uterine fibroids.
What are the Symptoms of an Inverted Uterus?
The clinical manifestations of an inverted uterus vary according to types and its classification as based on degree of its inversion or according to time of onset.
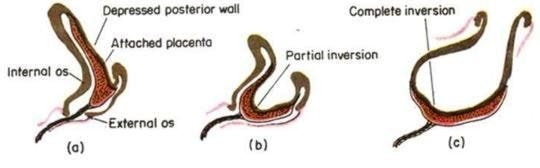
There are 2 main types:
- Partial uterine inversion – This is an incomplete inverted uterus, where it can only be seen within the area of the endometrial cavity, without reaching further beyond the external cervical os. .
- Complete uterine inversion – This is a complete inverted uterus, where it can be seen beyond the external cervical os.
Classification:
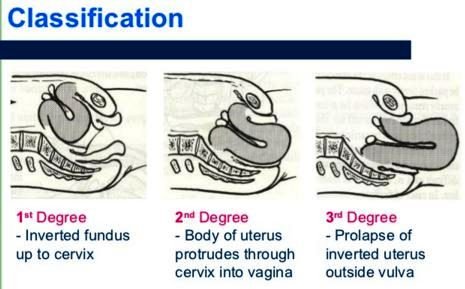
- First degree of inversion – The uterine inversion extends to, but not beyond the cervix.
- Second degree of inversion – The uterine inversion extends beyond the cervix, but stays within the vaginal area.
- Third degree of inversion or prolapsed inversion – The uterine inversion extends beyond the vaginal area.
- Total inversion or nonpuerperal inversion – This is mostly related with growth of a tumor and which involves the inversion of both the walls of the uterus and the vagina.
Onset of the inversion:
- Acute onset – This occurs prior to the contraction of the cervical ring, within 24 hours of delivery.
- Subacute onset – This is during the time of contraction of the cervical ring, beyond 24 hours of delivery until the 30th day postpartum.
- Chronic onset – This is seen after 4 weeks postpartum, which is specifically beyond the 30th day postpartum.
Specific signs and symptoms:
- Postpartal hemorrhage – This is an immediate problem of patients with an inverted uterus, who may experience massive bleeding and can end up into conditions of shock.
- Vaginal mass that suddenly appears – This is an alarming appearance of a large dark red mass that accompanies the placenta.
- Varying degrees of cardiovascular collapse – This accompanies cases of complete inversion.
What Causes an Inverted Uterus?
The exact cause of an inverted uterus is not yet known so far; although there are some predisposing conditions which might lead an individual person to have it and these are:
- Previous experience of uterine inversion
- Administration of magnesium sulfate at the time of labor
- Cases of placenta accreta and placenta previa
- Implantation of the placenta at the uterine fundus
- Application of forceful fundal pressure during delivery
- Umbilical cord is forcefully pulled out upon delivering the placenta
- Umbilical cord length is short and cord traction repeatedly applied
How is an Inverted Uterus Diagnosed?
The diagnosis of an inverted uterus is usually made depending upon the different signs and symptoms presented. It can be identified and confirmed through an ultrasound and magnetic resonance imaging.
Differential diagnosis can also be performed to point it out from the following conditions such as:
- Marked uterine atony during delivery
- Uterine tumor that is prolapsed
- Second twin that is undiagnosed
- Gestational trophoblastic disease noted
- An existing genital tract disease of a woman
How is an Inverted Uterus Treated?
The goal of medical management for an inverted uterus is directed at utilizing pharmacologic agents to correct uterine atony and replacing manually the uterus back with its normal position.
Principles of management are logically done in the following steps:
- Aggressive fluid replacement for hypotension and blood replacement for hypovolemia
- Uterine repositioning has to be done immediately when acute puerperal inversion is assessed
- Possible laparotomy
- Tocolytics to promote uterine contractions such Nitroglycerine IV, Terbutaline IV, Magnesium sulfate IV
- Manual reduction is performed through pushing the fundus in an upward direction until it’s in the normal position
- General anesthetic might be used and continue to manually manipulate using a fist by pushing the fundus upwards
- Bimanual uterine compression and gentle uterine massage
- Surgical approach through laparotomy/laparoscopy can be done when all else fails
- Oxytocic are given such as ergometrine, oxytocin or prostaglandins
- Antibiotics are started, uterine stimulants continued, closely monitor the patient after repositioning the uterus to prevent a re-inversion
References:
- Uterine Inversion : Epidemiology, Classification, Aetiology, Presentation, Differential diagnosis, Investigations, Management, Complications, Prognosis, References at http://patient.info/doctor/uterine-inversion
- http://www.medscape.com/viewarticle/405770_4
- http://www.merckmanuals.com/professional/gynecology-and-obstetrics/abnormalities-and-complications-of-labor-and-delivery/inverted-uterus
- Occhionero M, Restaino G, Ciuffreda M, et al. (2012). Uterine inversion in association with uterine sarcoma: a case report with MRI findings and review of the literature. Gynecol Obstet Invest; 73:260.
- Gomez-Lobo V, Burch W, Khanna PC (2007). Nonpuerperal uterine inversion associated with an immature teratoma of the uterus in an adolescent. Obstet Gynecol; 110:491.
- Lupovitch A, England ER, Chen R (2005). Non-puerperal uterine inversion in association with uterine sarcoma: case report in a 26-year-old and review of the literature. Gynecol Oncol; 97:938.