Fetal Distress
Definition
Fetal distress refers to an abnormal condition that happens in a pregnant woman, which might take place just before the time of delivery or during the childbirth process.
It is referred to as a non-reassuring fetal status by the American Congress of Obstetricians and Gynecologists, since fetal distress and birth asphyxia has been used interchangeably and more confusing, especially in confirming the diagnosis and with the proper management that is applicable for the problem.
Fetal distress has been confusingly used with the condition on birth asphyxia when the baby does not have the adequate amount of oxygen supply before labor, during the labor process or after the period of labor and delivery. The multiple possible causes of this can be due to low levels of oxygen present in the maternal blood, or there is an inadequate blood flow as a result of an umbilical cord compression.

It is historically used to describe a fetus that receives an insufficient amount of oxygen supply from the mother during the pregnancy period or at the moment of labor. Initial detection begins with an abnormal range of the fetal heart rate. This problem is noted approximately in 1 out of 20 pregnant women and fetal delivery has to happen just before any lasting clinical harm can be manifested.
Symptoms of Fetal Distress
The clinical manifestations of fetal distress are:
- Decreased fetal movement felt by the pregnant woman
- Presence of meconium in the amniotic fluid
- Intrauterine growth restriction
- Decreased variability noted in the monitoring of the fetal heart rate
- Fetal tachycardia or bradycardia
- Repetitive variable decelerations
- Late decelerations are noted
- Low biophysical profile
- Fetal metabolic acidosis present
- Elevation of fetal blood lactate levels
Causes
Uteroplacental insufficiency is considered as the main cause for antepartal fetal distress. The placenta is an important organ with a role in providing the enough amount of oxygen and nutrients through the umbilical cord going to the fetus.
Other causes of fetal distress are:
- Reduced uterine perfusion
- Breathing problems
- Multiple births
- Fetal abnormal position or presentation
- Shoulder dystocia noted during delivery
- Uteroplacental vascular disease
- Reduced fetal reserves
- Fetal sepsis during the pregnancy
- Nuchal cord
- Umbilical cord prolapse
- Abruptio placenta during labor
- Cases of uterine rupture
- Premature closure of the fetal ductus arteriosus
Fetal distress is associated with the following conditions:
- Maternal hypovolemia
- Fetal growth restriction
- Reduced liquor volume
Predisposing risk factors are women who have a history of:
- Multiple fetal pregnancies
- Stillbirth delivery
- Occurrence of polyhydramnios or oligohydramnios
- Cases of intrauterine growth restriction
- Hypertension during pregnancy, such as preeclampsia or eclampsia
- Rh sensitization problem
- Decreased fetal movements felt by the pregnant woman
- Cases of diabetes and other chronic conditions
- Pregnancy that is post-term
- Maternal age over 35 years old
Diagnosis
Attending physicians/obstetricians recommend the following for fetal distress:
- Ultrasound scan to observe for fetal movements and allow for an observation of the blood flow in the vessels that play the role in carrying blood from the placenta going to the fetus
- Electronic fetal heart rate monitoring to assess and evaluate the levels of hypoxia, monitor maternal uterine contractions, monitors the possibility for high risk deliveries
- Fetal acid base study to confirm fetal distress
- Fetal scalp blood sampling taken during the labor process to measure for the blood oxygen levels
- Regular examination of the amniotic fluid from the uterus in order to assess for some signs of meconium staining which can happen with fetal distress
Treatment
The treatment done is usually based on the different clinical manifestations of the patient during the assessment and evaluation done by members of the health team.
- Intrauterine resuscitation is considered as the primary treatment needed for a non-reassuring fetal status
- Rapid delivery by instrumental delivery is highly recommended among obstetricians
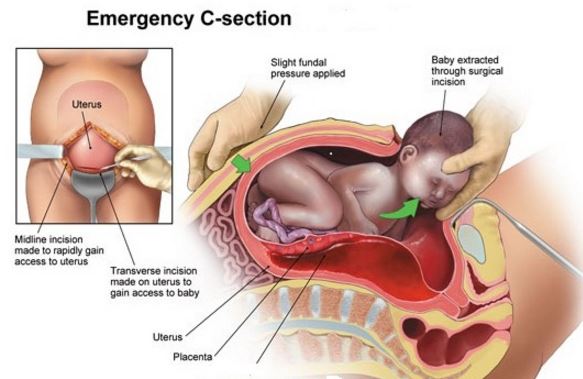
- Emergency cesarean birth in cases where vaginal delivery is not advised for the patient, or in cases of severe fetal distress and the presence of a cord prolapse
- Encouraging the mother to change position when lying down, specifically on a left lateral side-lying position
- The woman has to be well hydrated
- The woman has to be monitored for adequate oxygen supply
- Tocolysis to delay preterm labor of the woman by means of temporarily putting a stop to contractions
- Intravenous hypertonic dextrose fluid has to be started
- Amnioinfusion which involves fluid insertion into the amniotic cavity for the purpose of alleviating the compression of the umbilical cord
Complications
Some studies have shown that cases of fetal distress which are left untreated and not well managed can lead to brain damage of the fetus or worst is death.
References:
Fetal Distress: Diagnosis, Conditions & Treatment at http://americanpregnancy.org/labor-and-birth/fetal-distress/
Fetal Distress – Pathogenesis, Epidemiology, Presentation, Investigations, Management at http://patient.info/doctor/fetal-distress
http://www.aviva.co.uk/health-insurance/home-of-health/medical-centre/medical-encyclopedia/entry/fetal-distress/
Hofmeyr GJ, Lawrie TA (2012 Jan 18) Amnioinfusion for potential or suspected umbilical cord compression in labour. Cochrane Database Syst Rev. 1: CD000013.
Schauberger CW, Chauhan SP (2009 Mar). Emergency cesarean section and the 30-minute rule: definitions. Am J Perinatol. 26(3):221-6.
Graham EM, Ruis KA, Hartman AL, et al (2008 Dec). A systematic review of the role of intrapartum hypoxia-ischemia in the causation of neonatal encephalopathy. Am J Obstet Gynecol. 199(6): 587-95.