Velamentous Cord Insertion
Definition
Velamentous cord insertion abbreviated as VCI is an abnormal cord condition that happens during the pregnancy of a woman, in which the umbilical cord is noted to be inserted into the chorioamniotic membranes, as it travels within the membranes going to the placenta, just between the amnion and chorionic sites.
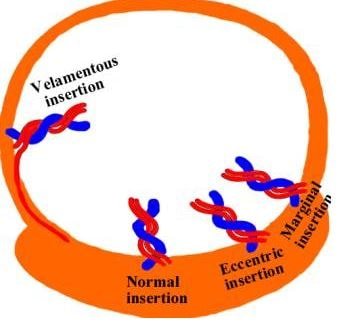
As the pregnancy develops, the umbilical cord is expected to normally insert itself in the middle portion of the placenta. Wharton’s jelly does not protect the remaining exposed vessels, placing it at risk for possible rupture.
Rupture is possible to happen when the blood vessels are located near the cervix, especially at the time of early labor process that might end up into a stillbirth delivery and this is referring to a condition called vasa previa. It has to be taken into account that not all cases of VCI leads to vasa previa; it is only occurring when the blood vessels are situated near the cervix of the woman.
The incidence of VCI is approximately 1% in a singleton pregnancy and about 9% for those experiencing twin pregnancies. It is more common among women who have placenta previa, as compared to those having the normal type of placental location. Its prevalence rate is a bit higher in cases of stillbirths from those who have multifetal pregnancies.
Symptoms of Velamentous Cord Insertion
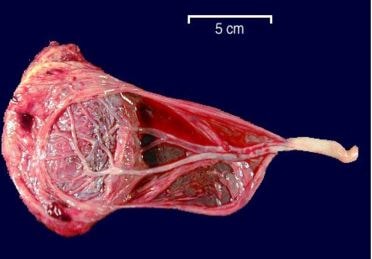
Velamentous cord insertion is being characterized by the presence of membranous umbilical vessels which are noted at the placental insertion site. The remainder part of the cord is usually taking a normal structure; these vessels are prone to incidence of compression and rupture as they are not being protected by Wharton’s jelly, especially if they are found to be covering the membranes of the cervical ostium such as in vasa previa condition.
The length of the membranous vessels greatly vary, the same as with the distance concerning the placental insertion and the end of the normal cord.
Causes
The umbilical cord is found to abnormally insert into the fetal membranes, specifically the chorioamniotic membranes, at the edge of the placental disk which is outside the placental margin, and then it is travelling within the membranes in reaching the placenta.
There are some proposed theories about the pathogenesis of VCI and these are:
- Trophotropism which is referring to a normal umbilical cord implantation that becomes abnormal, because of its central atrophy and the occurrence of some unidirectional lateral growth involving the chorion frondosum
- There is an abnormal primary implantation that took place as an end result of the embryonic obliquity during implantation period
- There is an abnormal fixation of the yolk sac to the chorion site, which is a distant site from the normal definitive placental site for growth
- The insertion of the body stalk occurs to a specific region of proliferating trophoblast, instead of the decidua basalis, so that the umbilical cord arises from a highly vascular chorion
VCI is associated with the following conditions:
- Placenta previa/vasa previa in women
- Cases of uterine anomalies
- Cases of bilobed placenta
- Presence of a single umbilical artery
- Increased incidence in multifetal pregnancies
- Intrauterine growth retardation
- Congenital anomalies of the fetus
- Preterm deliveries
- Low birth weight or fetuses that are considered small for gestational age
Diagnosis
Prenatal ultrasound can be performed to directly visualize the cord implantation that takes place at a site which is outside of the placenta.
- Ultrasonography has been used to finally diagnose cases of VCI either in the first trimester when possible, or mostly in the second trimester of the pregnancy
- Color Doppler imaging is used to specifically enhance the identification of the velamentous cord or vessels
VCI is also associated with having a result of a decreased level of the maternal serum alpha-fetoprotein and with a higher level of the maternal serum human chorionic gonadotropin
Treatment
The treatment for VCI usually relies on the specific location of the velamentous vessels.
Management can be done such as:
- Careful scanning in order to rule out the existence of fetal deformities
- Follow-up scans are usually scheduled to exclude a case of an intrauterine growth restriction
- Cervical dilatation can also be done when the need arises
- Once a velamentous cord insertion is being confirmed by an obstetrician, close monitoring is highly recommended to assess and evaluate for the presence of vasa previa
- Cesarean section type of delivery is done as early as 35 weeks age of gestation in cases when the blood vessels are assessed near the cervix to prevent the woman to go through the labor process, which might end up with stillbirth.
It has been taken into consideration that an early detection of a problem with velamentous cord insertion always minimizes the need for emergency cesarean birth.
Complications
The existing possible complications of velamentous cord insertion are:
- Cases of Type 1 vasa previa
- Increased risk for intrauterine growth restriction
- Increased risk for the occurrence of a twin to twin transfusion syndrome
- Increased risk for growth impairment in multifetal pregnancies
- Risk for intrapartum hemorrhage
- Risk for fetal bradycardia
- Fetal exsanguination as a result of ruptured vasa previa
Pictures

References:
http://radiopaedia.org/articles/velamentous-cord-insertion
http://emedicine.medscape.com/article/262470-overview#a4
http://www.fetalultrasound.com/online/text/34-034.htm
Weiner E, Fainstein N, Schreiber L, Sagiv R, Bar J, Kovo M. The association between umbilical cord abnormalities and the development of non-reassuring fetal heart rate leading to emergent cesarean deliveries. J Perinatol. 2015 Aug 20.
Lopriore E, Sueters M, Middeldorp JM, Oepkes D, Walther FJ, Vandenbussche FP. Velamentous cord insertion and unequal placental territories in monochorionic twins with and without twin-to-twin-transfusion syndrome. Am J Obstet Gynecol. 2007 Feb. 196(2):159.e1-5.
Hasegawa J, Matsuoka R, Ichizuka K, Sekizawa A, Okai T (March 2006). “Velamentous cord insertion: significance of prenatal detection to predict perinatal complications”. Taiwan J Obstet Gynecol 45 (1): 21–5.